I think that I am becoming a "healthcare professional"
I find myself frustrated with the lack of detail in my textbooks regarding..say...the endocrine system. I think that I have finally reached the "consciously incompetent" stage of being a paramedic. I am beginning to see that there are a ton of gaps in my knowledge.
I see that as a good thing.
I also have recently noticed that when I am getting information on a patient (from the patient, caregiver, nurse whatever) the wheels in my brain immediately begin spinning, and the next thing I know I am asking questions about pertinent information before I've even thought of it. Which I think is pretty cool.
Tuesday, December 20, 2011
Monday, December 19, 2011
The Oral Station
So, I used to play Dungeons and Dragons as a kid.
A few weeks ago, during one of the lab days in class, we began to work on an oral board type station.
Really all it was was playing Dungeons and Dragons...except there weren't any dungeons....or dragons...
Visualizing a situation in your head takes practice....luckily I had no trouble with it so far.
I have gone so far that during practical stations (during PALS in particular) I don't pay much attention to the simulated mannequin in front of me and just visualize everything in my brain...the outcomes tend to be better. I am definitely a lot more thorough that way.
I always had trouble with the practical stations, just because I was paying too much attention to what I saw with my eyes, I never thought to just play D and D with the situation. I barely passed the ITLS practical exam, because I was too busy being in the room with the dummy, and the examiner, and not being in my brain with the imaginary patient.
So go ahead, bust out the d20 and go slay some dragons...err..SAVE some patients...
update 7/12/12: Post about my experience in the Oral Station
A few weeks ago, during one of the lab days in class, we began to work on an oral board type station.
Really all it was was playing Dungeons and Dragons...except there weren't any dungeons....or dragons...
Visualizing a situation in your head takes practice....luckily I had no trouble with it so far.
I have gone so far that during practical stations (during PALS in particular) I don't pay much attention to the simulated mannequin in front of me and just visualize everything in my brain...the outcomes tend to be better. I am definitely a lot more thorough that way.
I always had trouble with the practical stations, just because I was paying too much attention to what I saw with my eyes, I never thought to just play D and D with the situation. I barely passed the ITLS practical exam, because I was too busy being in the room with the dummy, and the examiner, and not being in my brain with the imaginary patient.
So go ahead, bust out the d20 and go slay some dragons...err..SAVE some patients...
update 7/12/12: Post about my experience in the Oral Station
Sunday, December 18, 2011
So maybe thats why.....
Having not posted here in months for the simple reason that I have absolutely no time/mental energy to commit to such an endeavour as a blog.
So maybe thats why there are so few blogs about paramedic school.
So far, a good piece of advice that I can offer is that Cardiology isn't terrible if you truly understand the underlying physiology of things, and don't let Pediatrics sneak up on you.
Throughout Pediatrics there was an underlying mantra of "don't memorize, look it up"
The problem with that is to pass that module, memorizing normal heart rates of 3 month olds is necessary. Not to mention to pass the PALS written test.
Just an FYI...
But overall, I feel like I can see the light at the end of the tunnel. I have completely all my merit badges (ACLS, PALS, ITLS), as well as I have gotten all my intubations in the OR.
Just keep on truckin' I guess
So maybe thats why there are so few blogs about paramedic school.
So far, a good piece of advice that I can offer is that Cardiology isn't terrible if you truly understand the underlying physiology of things, and don't let Pediatrics sneak up on you.
Throughout Pediatrics there was an underlying mantra of "don't memorize, look it up"
The problem with that is to pass that module, memorizing normal heart rates of 3 month olds is necessary. Not to mention to pass the PALS written test.
Just an FYI...
But overall, I feel like I can see the light at the end of the tunnel. I have completely all my merit badges (ACLS, PALS, ITLS), as well as I have gotten all my intubations in the OR.
Just keep on truckin' I guess
Sunday, August 28, 2011
Advice for New Paramedics
I am always scanning the web for information for brandi-new and soon-to-be-brandi-new paramedics...
Rogue Medic posted a good piece about the differences between EMTs and Paramedics here
then again, if you are the kind of person (er...NERD!) that is searching out EMS blogs and whatnot...you probably have already been there.
Rogue Medic posted a good piece about the differences between EMTs and Paramedics here
then again, if you are the kind of person (er...NERD!) that is searching out EMS blogs and whatnot...you probably have already been there.
Saturday, August 27, 2011
A Clinical Episode...
So yesterday I was at the ED for clinical time...I am getting ready to start an IV on a patient. She was a woman in her 40s and her father was there. I introduced myself and set about finding a vein that was suitable. The patient father asks
"Are you ready for the hurricane?"
"Well, I bake my own bread and I don't drink milk, so I have no reason to rush out to the store..."
That was kind of a joke....I do bake bread and I don't drink milk, but it was suppose to be an observation of the absurdity of peoples actions when they hear of incoming natural disturbances...They all run out and buy milk and bread. But their response was somewhat suprising....
"You don't drink milk?" the patient said..
There was a harshness in her words that was unexpected for the mildly mannered folks they seemed to be. I told them that I do eat yogurt though. And they were immediately more at ease.
"Do you make your own yogurt?"
I told them I did, then the conversation moved on to using pasteurized milk vs. raw milk for yogurt. If I had ever tried Kefir and why do so many new aged crunchies have to buy cultures and starters through the mail and at Whole Foods that aren't really necessary. We also talked about how greek yogurt has gotten so popular and how it uses more milk.
I looked at them again. They were definitely rural folks, and realizing how dairy-centric the conversation had been, I went for a shot in the dark....
"Are you folks in the dairy business?"
Thank god I'm not lactose intolerant...Security may have to of been called.
"Are you ready for the hurricane?"
"Well, I bake my own bread and I don't drink milk, so I have no reason to rush out to the store..."
That was kind of a joke....I do bake bread and I don't drink milk, but it was suppose to be an observation of the absurdity of peoples actions when they hear of incoming natural disturbances...They all run out and buy milk and bread. But their response was somewhat suprising....
"You don't drink milk?" the patient said..
There was a harshness in her words that was unexpected for the mildly mannered folks they seemed to be. I told them that I do eat yogurt though. And they were immediately more at ease.
"Do you make your own yogurt?"
I told them I did, then the conversation moved on to using pasteurized milk vs. raw milk for yogurt. If I had ever tried Kefir and why do so many new aged crunchies have to buy cultures and starters through the mail and at Whole Foods that aren't really necessary. We also talked about how greek yogurt has gotten so popular and how it uses more milk.
I looked at them again. They were definitely rural folks, and realizing how dairy-centric the conversation had been, I went for a shot in the dark....
"Are you folks in the dairy business?"
Thank god I'm not lactose intolerant...Security may have to of been called.
Thursday, August 25, 2011
A window opens so I close the door...
So....Today is my last day at ForProfit Medical Transfer Company. Yesterday I accepted a per diem position at a local non-profit 911 service. The company does a fair amount of transfers out of the local hospitals...but they also do 911 in a pretty rural area, and the supervisor rotates everyone through the 911 shifts...which will be nice...becoming a paramedic never having done 911 was starting to make me nervous.
I start Tuesday...look forward to more clinical case studies of things I see in the field. Part of what spurred me to look for other work was that I wasn't seeing much of anything other than the steering wheel of a wheelchair transport truck in the last few months. Mostly due to the stubborn refusal of management to hire any EMTs for my station.
Onward...
I start Tuesday...look forward to more clinical case studies of things I see in the field. Part of what spurred me to look for other work was that I wasn't seeing much of anything other than the steering wheel of a wheelchair transport truck in the last few months. Mostly due to the stubborn refusal of management to hire any EMTs for my station.
Onward...
Tuesday, August 23, 2011
Success in Rhythm Recognition.....
The Key to Successful Rhythm Recognition is to have a rock solid understand about what all the little tracing represent in terms of vectors of electrical conduction through the heart. Its not about the heart beating....
At least that's how I think of it...and its worked for me pretty well..
At least that's how I think of it...and its worked for me pretty well..
Success in Clinicals
People will have different attitudes regarding Paramedics wherever you go. The response I have gotten from the ED has been overwhelmingly positive. Or at least....beige.
So far, my time in clinicals, I have met people who have been very glad to teach and give me opportunities. I have tried my hardest not to waste their time. I have met people that don't want anything to do with me...And I try my hardest to help them where I can, and show them that I am not there just to waste their time. I could be a snot or ignore those people, and re-enforce the attitudes that already exist. But I feel like I have found a really great site for clinicals, and I want to try my damnest that the paramedic students that come after me have at least as good an experience as I am, hopefully better. My educational experience doesn't exist in a vacuum, and my experience is colored by those that come before me, and my words and actions will affect those that come after me.
So far, my time in clinicals, I have met people who have been very glad to teach and give me opportunities. I have tried my hardest not to waste their time. I have met people that don't want anything to do with me...And I try my hardest to help them where I can, and show them that I am not there just to waste their time. I could be a snot or ignore those people, and re-enforce the attitudes that already exist. But I feel like I have found a really great site for clinicals, and I want to try my damnest that the paramedic students that come after me have at least as good an experience as I am, hopefully better. My educational experience doesn't exist in a vacuum, and my experience is colored by those that come before me, and my words and actions will affect those that come after me.
Tuesday, August 16, 2011
Why do I need an expensive stethoscope? Part II
So...If you didn't read my first opinion on expensive stethoscopes...read it here
Long story short, a few months ago...I thought I lost my scope...so I bought another...I bought a Littman Cardiology III, like clockwork, as soon as it arrived I found my old one.
A piece of advice that I try to live by is that one cannot possibly know the extend of one's ignorance. I didn't know how fine crackles can be...or how few places
"My scope is for blood pressures and lung sounds, and I don't have a problem hearing those things in the back of an ambulance with the cheap scope,..."
That was before I understood the difference between fine localized crackles, clear, and subtle wheezes....these things are harbingers of things to come...more importantly...they are harbingers of DIFFERENT things to come.
What a good paramedic hears for lung sounds will help her/him determine treatment. In which case I will do everything I possibly can to hear good lung sounds.
I still don't think EMT-Bs should be spending their money on expensive stethoscopes.
Long story short, a few months ago...I thought I lost my scope...so I bought another...I bought a Littman Cardiology III, like clockwork, as soon as it arrived I found my old one.
A piece of advice that I try to live by is that one cannot possibly know the extend of one's ignorance. I didn't know how fine crackles can be...or how few places
"My scope is for blood pressures and lung sounds, and I don't have a problem hearing those things in the back of an ambulance with the cheap scope,..."
That was before I understood the difference between fine localized crackles, clear, and subtle wheezes....these things are harbingers of things to come...more importantly...they are harbingers of DIFFERENT things to come.
What a good paramedic hears for lung sounds will help her/him determine treatment. In which case I will do everything I possibly can to hear good lung sounds.
I still don't think EMT-Bs should be spending their money on expensive stethoscopes.
Thursday, August 11, 2011

If dozens of hours in the ED has taught me anything...
We received a call to response to a possible stroke. On the way there, I called dispatch and asked if the nurse that called us told them when the patient began presenting with symptoms. She didn't know. I told my partner that "when the symptoms came on" was going to be the only question that the nurse had.
On scene we arrive, get a short history from the RN that called, after multiple attempts and finally establishing what the patient's baseline mental status was (See, I learned!). Symptoms started approx 3 minutes before. The patient had a GCS of 9, -1 eye, -3 verbal, -1 motor(is that how you are suppose to explain it?). But we were off to the ED. Once there, we transfer the patient who gets hooked up to all the monitors and whatnot...I give a history, my findings, and what the facility told me, then she asked...
"Do you know when the symptoms began?"
I thought I was the cat's pajamas until....
"Do you know the patient's code status?"
Damn, maybe next time. The patient didn't have the documentation we needed as EMTs to withhold resuscitation efforts, but that doesn't mean the patient is a full code either, and I didn't ask the nurse, because I was so certain that all that matter was when the symptoms came on, oh well....next time.
Other than the needle sticks, tubes, and drug pushes, my time in the ED has really taught me what the Nurses and Docs really want to know, and any way I can help facilitate that just makes their job easier and helps improve patient care. EMS gets tons of primary information about what is going on with the patient, we get to see what is happening where it is happening, and that makes for a much clearer clinical picture.
Wednesday, August 10, 2011
Don't touch anything Blue!!!
My instructor stated that the most stressful moment in your Paramedic Education is when you are called into to do your first tube in the Operating Room.
He was definitely right....
The RN firmly told me "Dont touch anything blue!" as I walked in.
The floor was blue, the patient was covered in blue sheets, everyone's scrubs were blue.
I quickly realized that she meant the person with the safety glasses and apron and sterile gloves, and the table covered in surgical instruments.
I didn't touch any of that stuff.
There was a MD anesthesiologist watching, but a CRNA was in charge of this patient. She asked if I had ever intubated anyone....I shook my head.
I wasn't sure if the patient was still awake...in retrospect, I am certain he was not.
She asked if I have intubated the mannikin. I nodded.
I opened the patient's mouth and was amazed at how little it looked at all like those plastic mannikins.
Eventually I found my bearings, and found my patient's larynx. I glanced up, and saw his oxygen stat was still at 100%.
The seal was cracked. One down....
He was definitely right....
The RN firmly told me "Dont touch anything blue!" as I walked in.
The floor was blue, the patient was covered in blue sheets, everyone's scrubs were blue.
I quickly realized that she meant the person with the safety glasses and apron and sterile gloves, and the table covered in surgical instruments.
I didn't touch any of that stuff.
There was a MD anesthesiologist watching, but a CRNA was in charge of this patient. She asked if I had ever intubated anyone....I shook my head.
I wasn't sure if the patient was still awake...in retrospect, I am certain he was not.
She asked if I have intubated the mannikin. I nodded.
I opened the patient's mouth and was amazed at how little it looked at all like those plastic mannikins.
Eventually I found my bearings, and found my patient's larynx. I glanced up, and saw his oxygen stat was still at 100%.
The seal was cracked. One down....
Thursday, July 21, 2011
And just like that....
...its July, and I just finished Mod 3.
To say that life has been busy is somewhat of an understatement. I throttled back the blog a hair just because its extremely difficult to understand what is important to a paramedic student while you are in the thick of it, only in retrospect, once you have surmounted an obstacle do you even grasp what was necessary to achieve it.
The big hurdle that I'm still climbing is IV therapy. Most of my education regarding that has come from the RNs at my clinical site. I started my ED time with exactly 2 live human sticks.
Right now I'm averaging slightly less that 50% success rate with IVs, but I am starting to understand what I am suppose to be doing more, and I learn something new with every stick.
It would have been nice to get some extra time from school with IV therapy, we have spent copious amounts of time on Patient Assessments and ET tubes, but whatever.
Its my opinion that the program that I am definitely has a weak link regarding the didactic stuff. Most of the training is done by "adjunct instructors" some of which are more helpful than others. There is a huge problem with consistency in message though. Often we are given conflicting information depending on who we are talking to, and the some of the instructors teach us to "pass the test" while others are teaching us to be good paramedics. Its somewhat annoying.
So we are beginning Cardiology next week...good times.
To say that life has been busy is somewhat of an understatement. I throttled back the blog a hair just because its extremely difficult to understand what is important to a paramedic student while you are in the thick of it, only in retrospect, once you have surmounted an obstacle do you even grasp what was necessary to achieve it.
The big hurdle that I'm still climbing is IV therapy. Most of my education regarding that has come from the RNs at my clinical site. I started my ED time with exactly 2 live human sticks.
Right now I'm averaging slightly less that 50% success rate with IVs, but I am starting to understand what I am suppose to be doing more, and I learn something new with every stick.
It would have been nice to get some extra time from school with IV therapy, we have spent copious amounts of time on Patient Assessments and ET tubes, but whatever.
Its my opinion that the program that I am definitely has a weak link regarding the didactic stuff. Most of the training is done by "adjunct instructors" some of which are more helpful than others. There is a huge problem with consistency in message though. Often we are given conflicting information depending on who we are talking to, and the some of the instructors teach us to "pass the test" while others are teaching us to be good paramedics. Its somewhat annoying.
So we are beginning Cardiology next week...good times.
Wednesday, April 6, 2011
Knocked off the High Horse...or Mod 2 Begins
So all last week I was floating along, imagining how much of a breeze class was going to be...because hey, I got a 91.4% on my Mod 1 Exam, right?
Well, my lack of studying definitely showed up in the first quiz of the next section....74.3%
I was particularly annoyed, because 3 questions out of 35 I was just careless, and wasn't paying attention. I didn't particularly do well on the first drug quiz either (oxygen). I really should have known that it wasn't my lack of understanding of the material that would be my downfall, but really my academic arrogance.
We have moved into the realm of pharmacology, which is awesome. Its amazing how much the Greek that I perused in my textbook is now coming together, as well as how much more I am understanding about what is going on with my patients at work.
I am trying to really get a solid understanding of these basic concepts if I hope to understand the stuff that we build on top of it. I would make some analogy about building foundations or something.
Well, my lack of studying definitely showed up in the first quiz of the next section....74.3%
I was particularly annoyed, because 3 questions out of 35 I was just careless, and wasn't paying attention. I didn't particularly do well on the first drug quiz either (oxygen). I really should have known that it wasn't my lack of understanding of the material that would be my downfall, but really my academic arrogance.
We have moved into the realm of pharmacology, which is awesome. Its amazing how much the Greek that I perused in my textbook is now coming together, as well as how much more I am understanding about what is going on with my patients at work.
I am trying to really get a solid understanding of these basic concepts if I hope to understand the stuff that we build on top of it. I would make some analogy about building foundations or something.
Thursday, March 31, 2011
Mod 1....in the Books
Its been a while since I've posted, just about after everything ramped up I lost all time to post. But last week was the Module 1 exam.
If I have it right, my paramedic program is designed into 10 separate modules. Each of which has quizzes and a test at the end. I guess this gives a much more representative sample of how a student is doing, instead of just one average for the whole class. Its obviously really important for a paramedic student to have a solid grasp on ALL the material, and this system keeps everyone on their toes, and makes sure that "The Well Being of the Paramedic" really doesn't carry as much weight as say....Cardiology.
Besides that, there is a pharmacology "class" that has quizzes that is a separate grade as well, for the same reason.
But the first (very low) hurdle has be stumbled over. A lot of the A and P stuff I have seen before, so it makes the concepts that are stacked on top of that easier.
Overall since we have now moved into Pharmacology, everything seems to fit together as a well designed system(imagine that?) so as long as I make sure that I am really understanding what is going on, and not just trying to memorize, things are moving fairly well.
If I have it right, my paramedic program is designed into 10 separate modules. Each of which has quizzes and a test at the end. I guess this gives a much more representative sample of how a student is doing, instead of just one average for the whole class. Its obviously really important for a paramedic student to have a solid grasp on ALL the material, and this system keeps everyone on their toes, and makes sure that "The Well Being of the Paramedic" really doesn't carry as much weight as say....Cardiology.
Besides that, there is a pharmacology "class" that has quizzes that is a separate grade as well, for the same reason.
But the first (very low) hurdle has be stumbled over. A lot of the A and P stuff I have seen before, so it makes the concepts that are stacked on top of that easier.
Overall since we have now moved into Pharmacology, everything seems to fit together as a well designed system(imagine that?) so as long as I make sure that I am really understanding what is going on, and not just trying to memorize, things are moving fairly well.
Tuesday, February 22, 2011
Put the Pedal to the Metal
And......Here we go....
Day four was heavy. The lecture was interdisciplinary with a focus on base concepts that we ABSOLUTELY HAVE TO UNDERSTAND to at all excel in the course and Paramedicine. It started out with some basic Cell structure/Microbiology, shifted to Chemistry, shifted to some Anatomy/Physiology, shifted to fluid balances and IV therapy, finishing off with the dreaded Acid/Base balance.
During one of the breaks, the instructor mentioned there is a shift towards requiring Anatomy and Physiology to become a Paramedic.
I completely agree with this direction. I'm sure that this stuff will be filled out as the course goes on, but learning about these different fields on a "need to know" basis, I don't think really makes for good education.
A lot of these concepts I remember covering in High School, so maybe I'm wrong.
Maybe its a wider societal opinion. It seems the attitude towards vocational education is something that you "get through" so that you can finally practice. I don't know why Paramedicine would be any different. And in part, it is sort of true. I'm fairly sure that I won't ever need to know that the cell membrane is composed of a phospholipid bi-layer. Maybe I'm just a nut because I am the type of person that just retains such information.
I am really excited that we are starting from the bottom up. After discussing intravascular pressure, I realized that malnourishment can cause edema. Maybe that was obvious or know by some readers already. But I'm glad that I was able to see that.
I already knew that albumin count in the blood was one of the ways that how well nourished a patient is measured.
Yesterday, I learned that it is large molecules like protein (albumin) that help water diffuse into the vascular system, due to their inability to pass through the cell wall.
I figured out that if a patient doesn't have enough albumin in their blood(malnourishment) then water will diffuse out of the vessels into the interstitial space causing....
Edema!!!
Where's my prize?
But anyway, I'm sorry if this is obvious, but it was relieving to know that I was able to take these parts of things that I am learning and able to use that knowledge critically, coming to new conclusions.
Which I think is really suppose to be the difference between a EMT and a Paramedic, its not just about the toys and drugs.
Day four was heavy. The lecture was interdisciplinary with a focus on base concepts that we ABSOLUTELY HAVE TO UNDERSTAND to at all excel in the course and Paramedicine. It started out with some basic Cell structure/Microbiology, shifted to Chemistry, shifted to some Anatomy/Physiology, shifted to fluid balances and IV therapy, finishing off with the dreaded Acid/Base balance.
During one of the breaks, the instructor mentioned there is a shift towards requiring Anatomy and Physiology to become a Paramedic.
I completely agree with this direction. I'm sure that this stuff will be filled out as the course goes on, but learning about these different fields on a "need to know" basis, I don't think really makes for good education.
A lot of these concepts I remember covering in High School, so maybe I'm wrong.
Maybe its a wider societal opinion. It seems the attitude towards vocational education is something that you "get through" so that you can finally practice. I don't know why Paramedicine would be any different. And in part, it is sort of true. I'm fairly sure that I won't ever need to know that the cell membrane is composed of a phospholipid bi-layer. Maybe I'm just a nut because I am the type of person that just retains such information.
I am really excited that we are starting from the bottom up. After discussing intravascular pressure, I realized that malnourishment can cause edema. Maybe that was obvious or know by some readers already. But I'm glad that I was able to see that.
I already knew that albumin count in the blood was one of the ways that how well nourished a patient is measured.
Yesterday, I learned that it is large molecules like protein (albumin) that help water diffuse into the vascular system, due to their inability to pass through the cell wall.
I figured out that if a patient doesn't have enough albumin in their blood(malnourishment) then water will diffuse out of the vessels into the interstitial space causing....
Edema!!!
Where's my prize?
But anyway, I'm sorry if this is obvious, but it was relieving to know that I was able to take these parts of things that I am learning and able to use that knowledge critically, coming to new conclusions.
Which I think is really suppose to be the difference between a EMT and a Paramedic, its not just about the toys and drugs.
Thursday, February 17, 2011
Day Three - ethice and glauco area
Ethics vs. Morals and CYA...er...legal liability is what we covered on the third day.
My effort to become more comfortable with medical terminology has also paid off because some of that was covered as well. My previous fluency in Spanish helps with the latin roots of stuff, sometimes...
We received our pharmacology manual, time to get started with the flash cards. Its exciting because the course is starting to ramp up.
Luckily I have had plenty of training on liability and legal issues jammed down my throat from Ski Patrol. I think the most important thing to remember is to do weigh the consequences of your actions before you do them, and try to imagine defending your actions in a court of law. But in the end, there is a lot of gray area, and you can't go wrong contacting medical control and documenting your actions well, I guess.
Part of the liability of a paramedic stems from being the highest level of provider typically on a scene, so not only are you liable for your own actions, but a paramedic can also be held liable for those who are working underneath him. So far, that leadership aspect has been mentioned but only in passing, maybe it will be covered more later on.
A few more quizzes came through, I updated my average.
Study habits have been mentioned as well, I guess I mentioned the importance of that some already.
My effort to become more comfortable with medical terminology has also paid off because some of that was covered as well. My previous fluency in Spanish helps with the latin roots of stuff, sometimes...
We received our pharmacology manual, time to get started with the flash cards. Its exciting because the course is starting to ramp up.
Luckily I have had plenty of training on liability and legal issues jammed down my throat from Ski Patrol. I think the most important thing to remember is to do weigh the consequences of your actions before you do them, and try to imagine defending your actions in a court of law. But in the end, there is a lot of gray area, and you can't go wrong contacting medical control and documenting your actions well, I guess.
Part of the liability of a paramedic stems from being the highest level of provider typically on a scene, so not only are you liable for your own actions, but a paramedic can also be held liable for those who are working underneath him. So far, that leadership aspect has been mentioned but only in passing, maybe it will be covered more later on.
A few more quizzes came through, I updated my average.
Study habits have been mentioned as well, I guess I mentioned the importance of that some already.
Tuesday, February 8, 2011
Day Two
Yesterday was the second day of class. We spent the whole day with a fitness/health specialist, discussing adequate nutrition and exercise. I have a lot of strong opinions about health and wellness based on my own personal experiences, the strongest of which is that there is a lot of bad information out there. But, he had a lot of good things to say. It was a change of pace for sure, because most of the time "wellness of the rescuer" type lectures tend to be just words, but we spent a lot of time doing simple exercises that could be done with minimal equipment.
The whole presentation was much more tailored for fire-fighters than paramedics, but then again, there are only so many exercises for lifting a stretcher into an ambulance.
I guess the guest-presenter is developing a health and wellness program for Public Service Workers, which I think is fantastic. There are plenty of perceptions out there about our field, most of them completely justified, that I think we all need to really work on.
One of his take home messages was that public safety workers really need to be more fit than professional athletes, because we will never know the "game" we will play, when we will play it, or for how long. His philosophy is definitely similar to Gym Jones or Crossfit but not nearly as intense. He had no love for "commercial gyms".
I like what he had to say about diet and nutrition. I find that it is so important to plan ahead if you want to eat well in this business, there's no other way about it.
We also took quizzes for Chapter 1, 2, and 3. I got a 90%, 94.3%, and 80%, respectively
The whole presentation was much more tailored for fire-fighters than paramedics, but then again, there are only so many exercises for lifting a stretcher into an ambulance.
I guess the guest-presenter is developing a health and wellness program for Public Service Workers, which I think is fantastic. There are plenty of perceptions out there about our field, most of them completely justified, that I think we all need to really work on.
One of his take home messages was that public safety workers really need to be more fit than professional athletes, because we will never know the "game" we will play, when we will play it, or for how long. His philosophy is definitely similar to Gym Jones or Crossfit but not nearly as intense. He had no love for "commercial gyms".
I like what he had to say about diet and nutrition. I find that it is so important to plan ahead if you want to eat well in this business, there's no other way about it.
We also took quizzes for Chapter 1, 2, and 3. I got a 90%, 94.3%, and 80%, respectively
Tuesday, February 1, 2011
Day One
It was really good.
It was spent like the first day of any class. The manager of the program (the guy who interviewed me) gave a little talk about expectations, then the main instructor explained who he was and his expectations, many opportunities were given to ask questions.
I like that policies and procedures regarding grades and attendance and everything was very well presented, and plenty of resources that were available were explained.
The educational philosphy of the school and the instructor was very much in line with what I believe, so I was really happy about that. The instructor said "This is Adult Education" no less than 4 times in the course of the day, which leads me to believe that his attitudes regarding some academic policies jive VERY well with my own.
Something that I found interesting was that they had the whole works split into separate "courses" so that if someone was very strong in the book work, but weak in pharmacology, then they wouldn't be able to squeeze by with a passing grade. Some folks may consider this harsh, but Medicine isn't a field that you want to screw around with, Emergency Medicine even less so.
I felt like the program is VERY much interested in establishing a core level of competency as a Paramedic, as opposed to just "teaching to the test".
I probably have the least time working on an ambulance, I guess we'll see how that goes. There was a good mix of folks from various areas and services, a lot of Southern New Hampshire and Boston. I might just buy and wear a Yankees cap just to be funny one day. But I should do that during baseball season for best response.
We covered the first three chapters in the book. There were powerpoint presentations, but luckily (unlike a lot of my college) the instructor didn't just read the slides, he kept the class relatively engaged.
There wasn't a lot of "war stories" either. Which is understandable, its kind of tough to get into those when discussing "the Well-Being of the EMT-P"
It was spent like the first day of any class. The manager of the program (the guy who interviewed me) gave a little talk about expectations, then the main instructor explained who he was and his expectations, many opportunities were given to ask questions.
I like that policies and procedures regarding grades and attendance and everything was very well presented, and plenty of resources that were available were explained.
The educational philosphy of the school and the instructor was very much in line with what I believe, so I was really happy about that. The instructor said "This is Adult Education" no less than 4 times in the course of the day, which leads me to believe that his attitudes regarding some academic policies jive VERY well with my own.
Something that I found interesting was that they had the whole works split into separate "courses" so that if someone was very strong in the book work, but weak in pharmacology, then they wouldn't be able to squeeze by with a passing grade. Some folks may consider this harsh, but Medicine isn't a field that you want to screw around with, Emergency Medicine even less so.
I felt like the program is VERY much interested in establishing a core level of competency as a Paramedic, as opposed to just "teaching to the test".
I probably have the least time working on an ambulance, I guess we'll see how that goes. There was a good mix of folks from various areas and services, a lot of Southern New Hampshire and Boston. I might just buy and wear a Yankees cap just to be funny one day. But I should do that during baseball season for best response.
We covered the first three chapters in the book. There were powerpoint presentations, but luckily (unlike a lot of my college) the instructor didn't just read the slides, he kept the class relatively engaged.
There wasn't a lot of "war stories" either. Which is understandable, its kind of tough to get into those when discussing "the Well-Being of the EMT-P"
Saturday, January 29, 2011
Learning Styles and the Paramedic Student
You will spend the rest of your life...
STUDYING!!!
I had a recent discussion with a soon to be finished paramedic student about what sort of time requirements were necessary to be successful in paramedic school. The vast majority of folks I come across speak of spending a lot of time studying. I think that stems from people's uncertainty about what type of learner they are.
I think a great disservice that is done to the vast majority of learners out there is not establishing a preferred learning style early on. I'll try to explain this better, so maybe this will help.
DISCLAIMER: This is a somewhat controversial model, but its the only one I have learned, in multiple fields. I guess maybe that is why it isn't widespread in the regular education system...
Wikipedia calls it Fleming's VAK/VARK Model. The idea is that everyone has a preferred method of disseminating information.
There are three methods:
A good teacher will incorporate every style into the lesson, but that doesn't help what a learner does on their own time.
Here is a quiz from AES education planner.Org for testing learning styles.
I think that if paramedic students are aware of their specific learning style, then it will be much easier for them to focus on how they should study, instead of wasting time.
While taking National Ski Patrol Instructor Development course I found out that the vast majority of Ski Patrollers are kinesthetic learners, and the majority of NSP's curriculum is geared towards that. I wouldn't be surprised to find that Emergency Medical Professionals are much the same way.
If that was the case, it would make sense for Paramedic Education to be difficult, because a lot of Medic school is....academic, for lack of a better word, and that kind of thing is definitely hard to teach kinesthetically. That would also explain why EMTs need to be taught that being a Medic is not about the skillz.
STUDYING!!!
I had a recent discussion with a soon to be finished paramedic student about what sort of time requirements were necessary to be successful in paramedic school. The vast majority of folks I come across speak of spending a lot of time studying. I think that stems from people's uncertainty about what type of learner they are.
I think a great disservice that is done to the vast majority of learners out there is not establishing a preferred learning style early on. I'll try to explain this better, so maybe this will help.
DISCLAIMER: This is a somewhat controversial model, but its the only one I have learned, in multiple fields. I guess maybe that is why it isn't widespread in the regular education system...
Wikipedia calls it Fleming's VAK/VARK Model. The idea is that everyone has a preferred method of disseminating information.
There are three methods:
- Auditory
- Visual
- Kinesthetic
A good teacher will incorporate every style into the lesson, but that doesn't help what a learner does on their own time.
Here is a quiz from AES education planner.Org for testing learning styles.
I think that if paramedic students are aware of their specific learning style, then it will be much easier for them to focus on how they should study, instead of wasting time.
While taking National Ski Patrol Instructor Development course I found out that the vast majority of Ski Patrollers are kinesthetic learners, and the majority of NSP's curriculum is geared towards that. I wouldn't be surprised to find that Emergency Medical Professionals are much the same way.
If that was the case, it would make sense for Paramedic Education to be difficult, because a lot of Medic school is....academic, for lack of a better word, and that kind of thing is definitely hard to teach kinesthetically. That would also explain why EMTs need to be taught that being a Medic is not about the skillz.
Thursday, January 27, 2011
The Application Process - Documentation
There is a lot of documentation involved with applying to a paramedic education program. No more or less really than any other college program, but definitely more than someone who expects to just walk in.
A Current Resume
How much does a resume matter in the scope of things when it comes to a job? It definitely says a lot when you don't have one. One ambulance service that I applied to twice (first time-no resume, second time-sent one) only called me back for an interview on the second instance, and they were even hiring. Resume skills are important in life in general. There is no standard about what makes a good resume, but for entry level positions, I'd say it is good to keep it to one page.
EMS Credentials
Kind of a given I guess.
Proof of Health Insurance
I was kind of suprised by this one, but luckily for where I live, health insurance is avaliable to everyone.
A Letter of Recommendation from the Head of my EMS service
They spelled my name wrong, I was definitely annoyed by this. I went to pick it up right before my interview, so I guess I can take the blame, but in the end, I guess it didn't matter.
Documentation of 50 calls as the primary responder over the past 12 months.
I guess this is a given as well, but if I was working as a volunteer for a a rural service one day a week, it might be a stretch.
A copy of my High School Diploma and College Transcripts(where applicable)
A lot of people aren't really "academic" which is okay, but to get through paramedic training, I think you need to have at least a basic level of academic proficiency and study habits, I will provide a post about learning styles this saturday.
This was a list of things that I was required to bring to the interview. But there was more...
A letter of recommendation from Medical Director of EMS service
I think that this was kind of meaningless, being that I have never met or seen the Med. Director of my service, but my program wanted this letter to state at least that there were no clinical issues that would keep me from finishing. Since my Medical Director isn't my PCP, I don't know how he/she would know this.
A Health Evaluation form
This had to be filled out by my PCP.
Proof of Childhood MMR immunizations
Also a given, working in Healthcare setting
Proof of Hep. B immunizations
Like I told the nurse at my PCP, I don't want some crackhead spitting blood in my face.
PPD test for TB
Another obvious one, I think its required by OSHA.
This was quite a list of things to compile, but if someone is working in Emergency Medicine already, it wouldn't be too bad.
A Current Resume
How much does a resume matter in the scope of things when it comes to a job? It definitely says a lot when you don't have one. One ambulance service that I applied to twice (first time-no resume, second time-sent one) only called me back for an interview on the second instance, and they were even hiring. Resume skills are important in life in general. There is no standard about what makes a good resume, but for entry level positions, I'd say it is good to keep it to one page.
EMS Credentials
Kind of a given I guess.
Proof of Health Insurance
I was kind of suprised by this one, but luckily for where I live, health insurance is avaliable to everyone.
A Letter of Recommendation from the Head of my EMS service
They spelled my name wrong, I was definitely annoyed by this. I went to pick it up right before my interview, so I guess I can take the blame, but in the end, I guess it didn't matter.
Documentation of 50 calls as the primary responder over the past 12 months.
I guess this is a given as well, but if I was working as a volunteer for a a rural service one day a week, it might be a stretch.
A copy of my High School Diploma and College Transcripts(where applicable)
A lot of people aren't really "academic" which is okay, but to get through paramedic training, I think you need to have at least a basic level of academic proficiency and study habits, I will provide a post about learning styles this saturday.
This was a list of things that I was required to bring to the interview. But there was more...
A letter of recommendation from Medical Director of EMS service
I think that this was kind of meaningless, being that I have never met or seen the Med. Director of my service, but my program wanted this letter to state at least that there were no clinical issues that would keep me from finishing. Since my Medical Director isn't my PCP, I don't know how he/she would know this.
A Health Evaluation form
This had to be filled out by my PCP.
Proof of Childhood MMR immunizations
Also a given, working in Healthcare setting
Proof of Hep. B immunizations
Like I told the nurse at my PCP, I don't want some crackhead spitting blood in my face.
PPD test for TB
Another obvious one, I think its required by OSHA.
This was quite a list of things to compile, but if someone is working in Emergency Medicine already, it wouldn't be too bad.
Uncovering Paramedic Clinicals
It is getting to be the countdown to the start of this show, and I was just looking around for some information about clinicals, and I came across this article:
Uncovering Paramedic Clinicals
It seems like it has some pretty good information.
Uncovering Paramedic Clinicals
It seems like it has some pretty good information.
Thursday, January 20, 2011
The Application Process - The Interview
The Interview and Skills Test
A few days after I had initially applied on line, I received an email with a specific date and time for my interview where the program was going to be held. Also attached was a list of the documentation that I needed to bring with me to the interview, as well as just a run down of what was going to happen.
The day of, I arrived fairly early, and the first step was the administrator of the program went over some of my documentation with me, and talked about the costs of the program, and how payment was expected up front, but they wouldn't mind making a payment plan as well, were they would charge a card monthly over the course of the program, which I thought was really great, because they didn't charge interest.
The program's refund policy is that they will pro-rate you a refund for however much of the class is left, if you can't finish it for whatever reason. So I'm sure as long as the student was "in the black" on their payments they wouldn't mind stretching things out a bit, which is really great, because the program costs $9000 before materials.
After I had a short discussion over costs, I was given a multiple choice test of EMT-B knowledge and a basic math/arithmetic test.
I wish I had gone over stuff a little bit before I took those tests, but I guess it doesn't matter now.
The math was all pretty straightforward, but I hadn't done any for a few years really, so I definitely spent some time cleaning out the cob-webs.
Afterwards, I had a discussion with the manager of the school. He talked about the school, and the hospital which is affiliated with it. He talked about the instructor I was going to have, he asked about any paramedics I knew, and what I liked about them. We went over the paperwork that I brought in. Any specific questions he asked me ("College? Anatomy and Physiology? Experience?") he had a check list for and he marked the answers, so I am guessing that part of the acceptance process is how many "points" you have on that sheet, I don't know if there is a minimum threshold or what, but I guess I did good enough.
We also took a tour of the facility. There were a few classrooms and some smaller skill labs. There was plenty of equipment to get familiar with, as well as a closet full of the drugs I would be learning about (except narcs). It was nice to see that the school had all the resources needed, right there, and there wasn't a need to "borrow" them from any hospital or fire department or whatever. I guess that is the kind of program I was looking for.
He also mentioned how many spots were open for the course, and I was surprised at how many applicants they had, but not really, being that there isn't a lot of options, like I said, in this area.
I made sure to show up with everything they had asked me to, and I was definitely dressed for an interview. I'm sure both of those things made a different, because talking to both staff members lead me to believe that a lot of folks don't really take the program's gravity seriously, and don't make it.
A few days after I had initially applied on line, I received an email with a specific date and time for my interview where the program was going to be held. Also attached was a list of the documentation that I needed to bring with me to the interview, as well as just a run down of what was going to happen.
The day of, I arrived fairly early, and the first step was the administrator of the program went over some of my documentation with me, and talked about the costs of the program, and how payment was expected up front, but they wouldn't mind making a payment plan as well, were they would charge a card monthly over the course of the program, which I thought was really great, because they didn't charge interest.
The program's refund policy is that they will pro-rate you a refund for however much of the class is left, if you can't finish it for whatever reason. So I'm sure as long as the student was "in the black" on their payments they wouldn't mind stretching things out a bit, which is really great, because the program costs $9000 before materials.
After I had a short discussion over costs, I was given a multiple choice test of EMT-B knowledge and a basic math/arithmetic test.
I wish I had gone over stuff a little bit before I took those tests, but I guess it doesn't matter now.
The math was all pretty straightforward, but I hadn't done any for a few years really, so I definitely spent some time cleaning out the cob-webs.
Afterwards, I had a discussion with the manager of the school. He talked about the school, and the hospital which is affiliated with it. He talked about the instructor I was going to have, he asked about any paramedics I knew, and what I liked about them. We went over the paperwork that I brought in. Any specific questions he asked me ("College? Anatomy and Physiology? Experience?") he had a check list for and he marked the answers, so I am guessing that part of the acceptance process is how many "points" you have on that sheet, I don't know if there is a minimum threshold or what, but I guess I did good enough.
We also took a tour of the facility. There were a few classrooms and some smaller skill labs. There was plenty of equipment to get familiar with, as well as a closet full of the drugs I would be learning about (except narcs). It was nice to see that the school had all the resources needed, right there, and there wasn't a need to "borrow" them from any hospital or fire department or whatever. I guess that is the kind of program I was looking for.
He also mentioned how many spots were open for the course, and I was surprised at how many applicants they had, but not really, being that there isn't a lot of options, like I said, in this area.
I made sure to show up with everything they had asked me to, and I was definitely dressed for an interview. I'm sure both of those things made a different, because talking to both staff members lead me to believe that a lot of folks don't really take the program's gravity seriously, and don't make it.
Saturday, January 15, 2011
Why the Jump?
also titled...
Why didn't I become an EMT-I before going into Paramedic School?
Lets look at some education guidelines...
For an EMT-B the education requirements are as follows....
that is per EMS.gov National Standards Cirricula
For an I-85(the intermediate level in New Hampshire)....
Okay...I searched and searched, and I can't get a straight answer out of anywhere about the hours of education and clinicals. The number of hours I typically saw was somewhere in the range of 200 or so for classroom time and clinicals, as well as a certain amount of IV sticks and intubations(where applicable). I guess in the range of 10 or so each. Please correct me if I'm wrong.
For my paramedic program...
So, let's visualize this...
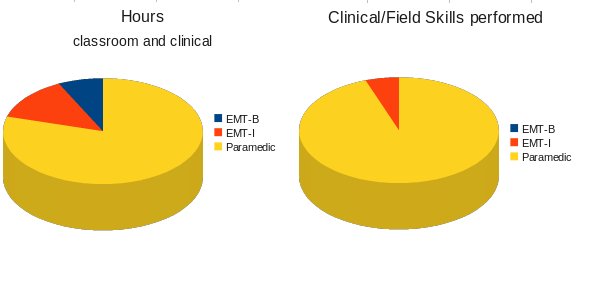
Finally, I found an interesting passage on pages 18-19 the DOT national standard curriculum for Paramedics(pdf file!) in regards to being a basic as a pre-requisite for Paramedic Education:
I guess I have confidence in my abilities and knowledge to complete the program and I thought going through with becoming an Intermediate first would just be a waste of my time and money. i feel like Paramedic Education goes so far above and beyond the intermediate level that any advantage would be overshadowed fairly quickly. Please comment if you agree or disagree.
Why didn't I become an EMT-I before going into Paramedic School?
Lets look at some education guidelines...
For an EMT-B the education requirements are as follows....
"In addition to the required 110 hours of instruction, this course requires that the student have patient interactions in a clinical setting."
that is per EMS.gov National Standards Cirricula
For an I-85(the intermediate level in New Hampshire)....
Okay...I searched and searched, and I can't get a straight answer out of anywhere about the hours of education and clinicals. The number of hours I typically saw was somewhere in the range of 200 or so for classroom time and clinicals, as well as a certain amount of IV sticks and intubations(where applicable). I guess in the range of 10 or so each. Please correct me if I'm wrong.
For my paramedic program...
So, let's visualize this...
Finally, I found an interesting passage on pages 18-19 the DOT national standard curriculum for Paramedics(pdf file!) in regards to being a basic as a pre-requisite for Paramedic Education:
EMT-Basic
It has been a long held tradition to use EMT-Basic certification as a prerequisite for more advanced EMS education, and this curriculum continues that tradition. It is important to note that some educators have questioned the practice of using EMT-Basic as a required certification prior to enrollment in Paramedic education. In fact, no studies have been able to verify EMT-Basic certification or experience as a predictor of success in paramedic education. Of course, paramedics are required to be competent in all of the skills and knowledge of and EMT-Basic, and this knowledge base and skills competence should be verified during paramedic education.
Although this curriculum identifies EMT-Basic as a prerequisite, we have done so in the absence of empirical data suggesting that this is appropriate. We encourage flexibility in approaching the issue of EMT-Basic as a prerequisite to paramedic education. We also recognize that it may be possible to incorporate all of the material of an EMT-Basic class into a paramedic program, eliminating the need for it as a prerequisite. Clearly, more research is needed.
{kind=link}
I guess I have confidence in my abilities and knowledge to complete the program and I thought going through with becoming an Intermediate first would just be a waste of my time and money. i feel like Paramedic Education goes so far above and beyond the intermediate level that any advantage would be overshadowed fairly quickly. Please comment if you agree or disagree.
Wednesday, January 12, 2011
The Application Process - The Beginning
Since I still have a few weeks before things get started, I figure I can talk about what the application process was like for the Paramedic Program I am enrolled in.
How did I pick my program?
I didn't have many choices living where I do, but I knew I didn't want to get involved with a Community College based program, because years ago I took an EMT-B class as a CC, and wasn't very happen with the outcomes, I never took the National Registry test then, because I was out of the country at the time, and I really don't think I had the maturity level to be working in healthcare at the time (I know right?). I also already have an Associate's and a Bachelor's degree, so I was really only interested in getting my paramedic education. I didn't need any more pieces of paper.
Scheduling was also an issue, my program meets one day a week, and I can schedule clinicals around my work schedule. The school is also a 2.5 hour drive, so only making that once a week is definitely better for me.
I also took my EMT-B at a place that was specifically in the business of EMS training, and I was happy with the outcomes of the program, it was definitely more expensive, but the instructors were full-time instructors, and we were able to take the National Registry test at the school, using the equipment that we were familiar and practicing with.
Once I chose what program I was going to do, there was quite a list of things that I had to do, and I will go over them one by one.
Preliminary Application
This application was quick and easy, my national registry number and basic information (address, phone, etc). I think it was a $75 application fee
This was done all on line, through the Program's website.
I will post about the Interview process, as well as all the documentation I needed later.
How did I pick my program?
I didn't have many choices living where I do, but I knew I didn't want to get involved with a Community College based program, because years ago I took an EMT-B class as a CC, and wasn't very happen with the outcomes, I never took the National Registry test then, because I was out of the country at the time, and I really don't think I had the maturity level to be working in healthcare at the time (I know right?). I also already have an Associate's and a Bachelor's degree, so I was really only interested in getting my paramedic education. I didn't need any more pieces of paper.
Scheduling was also an issue, my program meets one day a week, and I can schedule clinicals around my work schedule. The school is also a 2.5 hour drive, so only making that once a week is definitely better for me.
I also took my EMT-B at a place that was specifically in the business of EMS training, and I was happy with the outcomes of the program, it was definitely more expensive, but the instructors were full-time instructors, and we were able to take the National Registry test at the school, using the equipment that we were familiar and practicing with.
Once I chose what program I was going to do, there was quite a list of things that I had to do, and I will go over them one by one.
- Preliminary Application
- Interview/Testing
- Documentation
Preliminary Application
This application was quick and easy, my national registry number and basic information (address, phone, etc). I think it was a $75 application fee
This was done all on line, through the Program's website.
I will post about the Interview process, as well as all the documentation I needed later.
Saturday, January 8, 2011
Wilderness Medicine....

is where I started.
I began my journey in Emergency Medicine by taking a Wilderness First Responder Course taught by by Stonehearth Open Learning Opportunities.
My definition of Wilderness Medicine is:
The assessment and treatment of patients in situations where transportation to definitive care is not readily accessible
Just consider any instance where "the golden hour" is definitely not going to be an option.
It has definitely affected my attitudes and beliefs towards patient care.
It has helped me understand that Emergency Medicine is all about looking for trends and treating problems before they become problems. Emergency Medicine is about understand what's really important (AIRWAY! AIRWAY! AIRWAY!!) and understanding how seemingly secondary injury may exacerbate what we really should be paying attention to.
In the urban world, sometimes when talking to colleagues I refer to "hot potato-ing" a patient. Typically this is in jest, but I am a firm believer that in most instances there is nothing I can really do to make a patient better, and my job as a basic rescuer involves trying to keep the patient from getting worst before I can "hot potato" them to the next level of definitive care.
This attitude really doesn't work so well for Paramedics.
If a patient goes into cardiac arrest, there really isn't anything a hospital can do for them that a paramedic can't (as far as I know). And I think that this is where much of the difficulty of that mindset swap may throw some wannabe-student-paramedics off, because if they spent their entire previous work history constantly hot potato-ing patients off, then actually dealing with a stressful situation may be difficult, if not impossible.
Wilderness Medicine is the exact opposite.
From minute one, you are taught that this situation is going to be long, and no way is this patient going to be going anywhere soon.
So we will see how things go I guess.
Tuesday, January 4, 2011
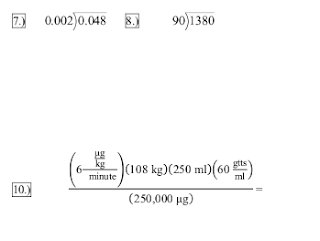
Med Math...er...Arithmetic..
I got an email from my instructor a few days ago, included was a few practice problems that we were expected to be comfortable with.
I looked at them, and immediately I thought about all the upper levels of Calculus and Discrete Mathematics I had encountered completing my Computer Science degree.
My ego scoffed at how easy it was, and that it wasn't math, but simple arithmetic...
I started working on the problems, and luckily, I was able to find instructions for long division on the internet.
I think that I will have to be careful, because sometimes I have the tendency to trivialize things that I had exposure to in the past, without actually assessing my competency in them. I guess that might not be right, because I was in the process of assessing when I realized that I completely forgot how to do long division.
But luckily, when it got to the scary looking stuff, I did alright...I think. The units I ended up with were an actual measurement, so that's pretty exciting.
At least I think I did...if anyone solves these problems, feel free to leave your answer in the comments, I'll share what I got too.
I looked at them, and immediately I thought about all the upper levels of Calculus and Discrete Mathematics I had encountered completing my Computer Science degree.
My ego scoffed at how easy it was, and that it wasn't math, but simple arithmetic...
I started working on the problems, and luckily, I was able to find instructions for long division on the internet.

I think that I will have to be careful, because sometimes I have the tendency to trivialize things that I had exposure to in the past, without actually assessing my competency in them. I guess that might not be right, because I was in the process of assessing when I realized that I completely forgot how to do long division.
But luckily, when it got to the scary looking stuff, I did alright...I think. The units I ended up with were an actual measurement, so that's pretty exciting.
At least I think I did...if anyone solves these problems, feel free to leave your answer in the comments, I'll share what I got too.
Saturday, January 1, 2011
Weigh the consequences....
Is it bad to over-react in Emergency Medicine?
I came on the scene, the patient was lying prone in firm snow, on a fairly steep bank on the uphill side of a trail. His right ski was still on his foot, and his left boot was externally rotated to what appeared to be opposite of the bend in the knee. Neither of his ski boots were buckled correctly, and consequence of such, were very loose. He was relatively calm, probably about 10 years old. I asked him what happened...
He said that he had fallen and twisted his ankle, and now it felt "weird". He said he couldn't walk on it. He used words like tingling, burning, electricity, numbness. The patient denied other injuries and there was no spinal point tenderness on palpation. The position he was in, plus the possibility of an in-boot spiral tib/fib were my main concerns. I tried to palpate for deformity/open wounds in his boot. After a slight scare that turned into melted snow, I ruled out any bleeding, but I couldn't tell on deformities one way or the other.
I called for a backboard and a set of hands because the patient was in relative comfort in the position found, and I didn't want to have to flip him, and end up have him screaming as his leg flopped around, or both of us go sliding down the hill and cause more significant injury to his leg.
When help arrived, we managed to log roll the patient onto the backboard, which caused no discomfort at all, the patients injured foot was stable, and didn't rotate to either direction. After more assessment I finally asked the right question...
"Have you ever hurt yourself before?"
"Yeah, but I've never broken anything, just bruises"
"How much does your ankle hurt compared to that?"
"Less..."
We took him off the board, he sat up, and we got him down, he walked just fine.
If I just went on the level of discomfort this patient was in, I could have figured he just twisted his ankle. But I had been in a similar situation; the EMTs were certain I didn't break my femur because I wasn't screaming enough. I'm sure they had learned in the back room of some fire house that femur injuries hurt like hell and the patient will be screaming their bloody cords out. There are so many subjective measures in what we do, the only thing that we can do is what we think is best for the patient at the time.
On scene, for a moment, I was slightly worried about overreacting, for a split second I was concerned what folks would say for me calling for a backboard for a patient with a twisted ankle, but I am glad that I immediately thought about what would happen to this patient did have a fracture, and if I did try to flip them on my own and take care of the situation without help. There would be a chance that we would have slipped a few dozen feet down the slope.
As I read over this post, and think about this situation I guess if I had asked the patient if they could flip on to their back or sit up, he would have, and been fine, but I assumed that no one would lie face down in the snow unless that WAS the most comfortable position, but I guess the way his leg was presenting put that out of my mind right away. I guess you can call that defensive assumptions.
One thing I know for certain is that I can only do what I think is best for the patient at that moment in time. It is easier to justify our actions for the worst case scenario than to say "I didn't think it was that bad"
As I read over this post, and think about this situation I guess if I had asked the patient if they could flip on to their back or sit up, he would have, and been fine, but I assumed that no one would lie face down in the snow unless that WAS the most comfortable position, but I guess the way his leg was presenting put that out of my mind right away
I came on the scene, the patient was lying prone in firm snow, on a fairly steep bank on the uphill side of a trail. His right ski was still on his foot, and his left boot was externally rotated to what appeared to be opposite of the bend in the knee. Neither of his ski boots were buckled correctly, and consequence of such, were very loose. He was relatively calm, probably about 10 years old. I asked him what happened...
He said that he had fallen and twisted his ankle, and now it felt "weird". He said he couldn't walk on it. He used words like tingling, burning, electricity, numbness. The patient denied other injuries and there was no spinal point tenderness on palpation. The position he was in, plus the possibility of an in-boot spiral tib/fib were my main concerns. I tried to palpate for deformity/open wounds in his boot. After a slight scare that turned into melted snow, I ruled out any bleeding, but I couldn't tell on deformities one way or the other.
I called for a backboard and a set of hands because the patient was in relative comfort in the position found, and I didn't want to have to flip him, and end up have him screaming as his leg flopped around, or both of us go sliding down the hill and cause more significant injury to his leg.
When help arrived, we managed to log roll the patient onto the backboard, which caused no discomfort at all, the patients injured foot was stable, and didn't rotate to either direction. After more assessment I finally asked the right question...
"Have you ever hurt yourself before?"
"Yeah, but I've never broken anything, just bruises"
"How much does your ankle hurt compared to that?"
"Less..."
We took him off the board, he sat up, and we got him down, he walked just fine.
If I just went on the level of discomfort this patient was in, I could have figured he just twisted his ankle. But I had been in a similar situation; the EMTs were certain I didn't break my femur because I wasn't screaming enough. I'm sure they had learned in the back room of some fire house that femur injuries hurt like hell and the patient will be screaming their bloody cords out. There are so many subjective measures in what we do, the only thing that we can do is what we think is best for the patient at the time.
On scene, for a moment, I was slightly worried about overreacting, for a split second I was concerned what folks would say for me calling for a backboard for a patient with a twisted ankle, but I am glad that I immediately thought about what would happen to this patient did have a fracture, and if I did try to flip them on my own and take care of the situation without help. There would be a chance that we would have slipped a few dozen feet down the slope.
As I read over this post, and think about this situation I guess if I had asked the patient if they could flip on to their back or sit up, he would have, and been fine, but I assumed that no one would lie face down in the snow unless that WAS the most comfortable position, but I guess the way his leg was presenting put that out of my mind right away. I guess you can call that defensive assumptions.
One thing I know for certain is that I can only do what I think is best for the patient at that moment in time. It is easier to justify our actions for the worst case scenario than to say "I didn't think it was that bad"
As I read over this post, and think about this situation I guess if I had asked the patient if they could flip on to their back or sit up, he would have, and been fine, but I assumed that no one would lie face down in the snow unless that WAS the most comfortable position, but I guess the way his leg was presenting put that out of my mind right away
Subscribe to:
Posts (Atom)